In any diagnostic laboratory, the Complete Blood Count (CBC) is the most frequently ordered test. It tells clinicians about red blood cells, white blood cells, and platelets — providing critical insight into infection, anemia, clotting disorders, leukemia, and dozens of other conditions. The machine at the center of every CBC workflow is the hematology analyzer, and not all hematology analyzers are created equal.
At Medlogics, we have deployed Laboratory Information System (LIS) integrations across diagnostic centers in Bangladesh, connecting our platform to a wide range of hematology analyzers — from compact 3-part machines in rural upazila health complexes to advanced 5-part analyzers in urban tertiary hospitals. Understanding the difference between these two classes of instruments is essential for any laboratory administrator, pathologist, or IT team managing a diagnostic facility.
What Does a Hematology Analyzer Actually Measure?
A hematology analyzer processes a small volume of anticoagulated blood and counts, measures, and characterizes blood cells at high speed. The core outputs of any hematology analyzer are:
- RBC count — Red blood cell concentration, hemoglobin level, hematocrit (HCT), MCV, MCH, MCHC, RDW
- WBC count — Total white blood cell count, and the critical differential — breaking that count into specific white cell types
- Platelet count — PLT concentration, MPV (mean platelet volume)
The key differentiating factor between machine classes is how deeply the WBC differential is performed. This is where the 3-part and 5-part distinction comes in.
The 3-Part Differential Analyzer

A 3-part differential (also called a 3-diff) analyzer classifies white blood cells into three broad categories using electrical impedance (cell size and volume):
- Lymphocytes — small, round cells (B-cells, T-cells, NK cells)
- Mid-range cells (MID) — monocytes, eosinophils, basophils grouped together
- Granulocytes — neutrophils and any large granular cells
The technology is elegant in its simplicity. Because 3-diff machines rely primarily on impedance (cell size), they are less expensive to manufacture, easier to maintain, require less reagent, and perform reliably in environments where humidity control, power stability, and technical expertise may be limited.
Common 3-Part Differential Machines


Typical use cases: Rural diagnostic centers, upazila-level health complexes, small urban clinics, point-of-care facilities where throughput is moderate and the clinical question is whether white cells are broadly elevated or shifted — not the specific subtype breakdown.
Limitation: A 3-diff machine cannot reliably distinguish neutrophils from eosinophils or basophils. For a patient with suspected eosinophilia, parasitic infection, or an allergic response where eosinophil percentage matters clinically, a 3-diff result will miss or underreport this. Any abnormal flag from a 3-diff typically requires a manual peripheral blood smear review by a pathologist — or referral to a 5-diff lab.
The 5-Part Differential Analyzer

A 5-part differential (5-diff) analyzer classifies white blood cells into five distinct populations with high accuracy by combining multiple detection technologies — typically impedance, radiofrequency (RF), and laser-based light scatter (flow cytometry principles). This allows the machine to individually quantify:
- Neutrophils (NEU) — the primary responders to bacterial infection
- Lymphocytes (LYM) — central to viral immune responses
- Monocytes (MONO) — large phagocytic cells, elevated in chronic infection and some malignancies
- Eosinophils (EOS) — elevated in allergic reactions, asthma, and parasitic infections
- Basophils (BASO) — rare cells, elevated in certain leukemias and allergic states
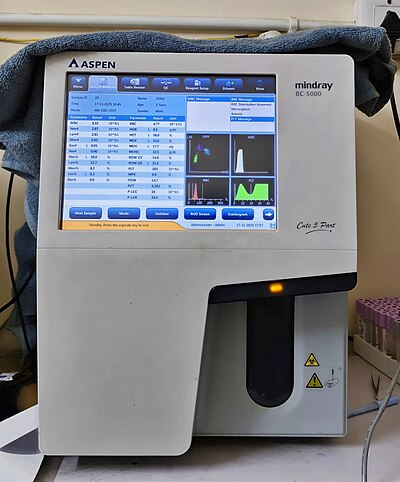
Advanced 5-diff machines also generate additional flags and scattergrams — visual representations of cell populations — that allow pathologists to spot abnormal cell morphology, blasts (early leukemia indicator), immature granulocytes, and nucleated RBCs without performing a manual smear in most cases.
Common 5-Part Differential Machines




Typical use cases: Urban multi-specialty hospitals, tertiary diagnostic centers, oncology and hematology departments, facilities that require ImmGen (immature granulocyte) reporting, and any lab where the clinician needs actionable subtype data rather than a screening result.
3-Part vs. 5-Part: At a Glance
| Feature | 3-Part Differential | 5-Part Differential |
|---|---|---|
| WBC categories reported | Lymphocytes, MID, Granulocytes | Neutrophils, Lymphocytes, Monocytes, Eosinophils, Basophils |
| Technology | Electrical impedance | Impedance + RF + Laser / Flow cytometry |
| Identifies eosinophilia | ❌ Not reliably | ✅ Yes |
| Detects blast flags | Limited | ✅ Advanced flagging + scattergrams |
| Throughput (typical) | 60–80 samples/hr | 80–200+ samples/hr |
| Cost | Lower capital + running cost | Higher initial investment |
| Best setting | Small labs, rural, primary care | Hospital labs, referral centers, oncology |
| Manual smear needed | More often flagged for review | Less often — automated morphology flags |
How Medlogics Integrates Both Machine Types

The practical challenge for any diagnostic lab running Medlogics is not whether a machine is 3-diff or 5-diff — it is whether the results flow automatically from the analyzer into the patient report without manual transcription. This is where Medlogics LIS integration delivers its core value.
Medlogics connects to hematology analyzers using two industry-standard communication protocols:
- ASTM E1381 / ASTM E1394 — the serial/RS-232 protocol used by older and mid-range analyzers. Most 3-diff machines and older 5-diff machines support ASTM. The analyzer sends results as structured text; Medlogics parses and maps these to the patient’s CBC order automatically.
- HL7 v2.x (ORU^R01 messages) — the IP-based messaging standard used by newer, networked analyzers. When a Sysmex XN Series or Mindray BC-6800 completes an analysis, it sends an HL7 ORU message over TCP/IP to the Medlogics middleware engine, which validates, routes, and commits the result to the patient record in real time.
Both connection types support bidirectional workflow: Medlogics not only receives results from the analyzer — it also sends the patient demographics and test order to the analyzer when the sample is received. This eliminates one of the most common sources of error in diagnostic labs: manual patient ID entry on the machine keypad.
Analyzers Currently Integrated with Medlogics
- Sysmex KX-21N, XT-2000i, XT-4000i, XN-1000, XN-2000, XN-3000
- Mindray BC-3000 Plus, BC-3600, BC-5300, BC-5500, BC-5800, BC-6800
- Beckman Coulter LH 750, LH 780, DxH 500, DxH 800, DxH 900
- Abbott Cell-Dyn 1800, Cell-Dyn 3700, Cell-Dyn Ruby, CELL-DYN Sapphire
- Horiba Micros 60, Pentra 60, Pentra 80, Yumizen H500, Yumizen H550
- Nihon Kohden MEK-6318, MEK-6410, MEK-7222
- Roche Cobas m 511
When a result lands in Medlogics, it is already matched to a patient, validated against reference ranges, flagged for abnormals, and ready for pathologist authorization — in seconds, not minutes.
The Impact in the Field: Bangladesh
In diagnostic centers across Dhaka, Chittagong, and Rangpur where Medlogics has been deployed, the shift from manual result entry to automated analyzer integration has had measurable effects:
- Transcription errors dropped to zero on integrated analyzers. Manual entry of 14–22 CBC parameters per test was a significant source of data errors under high-volume conditions.
- Report turnaround time (TAT) decreased by 40–60% in labs moving from manual to automated LIS-integrated workflows.
- Pathologist authorization became faster. With structured result data, reference ranges, and abnormal flags pre-populated by the LIS, pathologists review and release results with greater speed and confidence.
Whether your lab runs a compact Mindray BC-3000 or a high-throughput Sysmex XN-3000 — if it connects to Medlogics, the result flows automatically, the patient record stays complete, and your staff focuses on clinical work, not data entry.
Md. Tarikul Islam is a Laboratory Systems Analyst at Medlogics, based in Dhaka, Bangladesh. He has led LIS integration projects for over 40 diagnostic laboratories across Bangladesh and has trained more than 200 lab technicians on digital workflow adoption.